FREQUENCY OF NEW ONSET RIGHT BUNDLE BRANCH BLOCK IN ACUTE MYOCARDIAL INFARCTION
DOI:
https://doi.org/10.71000/mx0m8247Keywords:
Acute Myocardial Infarction, Right Bundle Branch Block, ECG, Cardiac Conduction, RBBB, Ischemic Heart Disease, Cross-Sectional Study. , Electrocardiography,Abstract
Background: Acute Myocardial Infarction (AMI) remains a critical cardiovascular emergency frequently associated with conduction disturbances, including Right Bundle Branch Block (RBBB). The sudden onset of RBBB during AMI not only complicates electrocardiographic interpretation by masking ischemic changes but may also correlate with worse clinical outcomes such as arrhythmias and heart failure. Despite its clinical importance, limited local data exist regarding the frequency and characteristics of new-onset RBBB among AMI patients, highlighting a gap in regional cardiac research.
Objective: To determine the frequency of new-onset Right Bundle Branch Block in patients presenting with Acute Myocardial Infarction.
Methods: This descriptive cross-sectional study was carried out at the Department of Cardiology, Lady Reading Hospital, Peshawar, over a six-month period. A total of 131 patients aged 18 to 60 years, diagnosed with AMI based on standardized criteria, were enrolled using non-probability consecutive sampling. Patients with previously diagnosed RBBB, cardiac surgery, electrolyte abnormalities, or pregnancy were excluded. Standard 12-lead ECGs were performed on admission, and RBBB was identified by a QRS duration >120 milliseconds and an rSR′ pattern in lead V1. Data were analyzed using SPSS version 26, with chi-square or Fisher’s exact test applied for stratification. A p-value <0.05 was considered statistically significant.
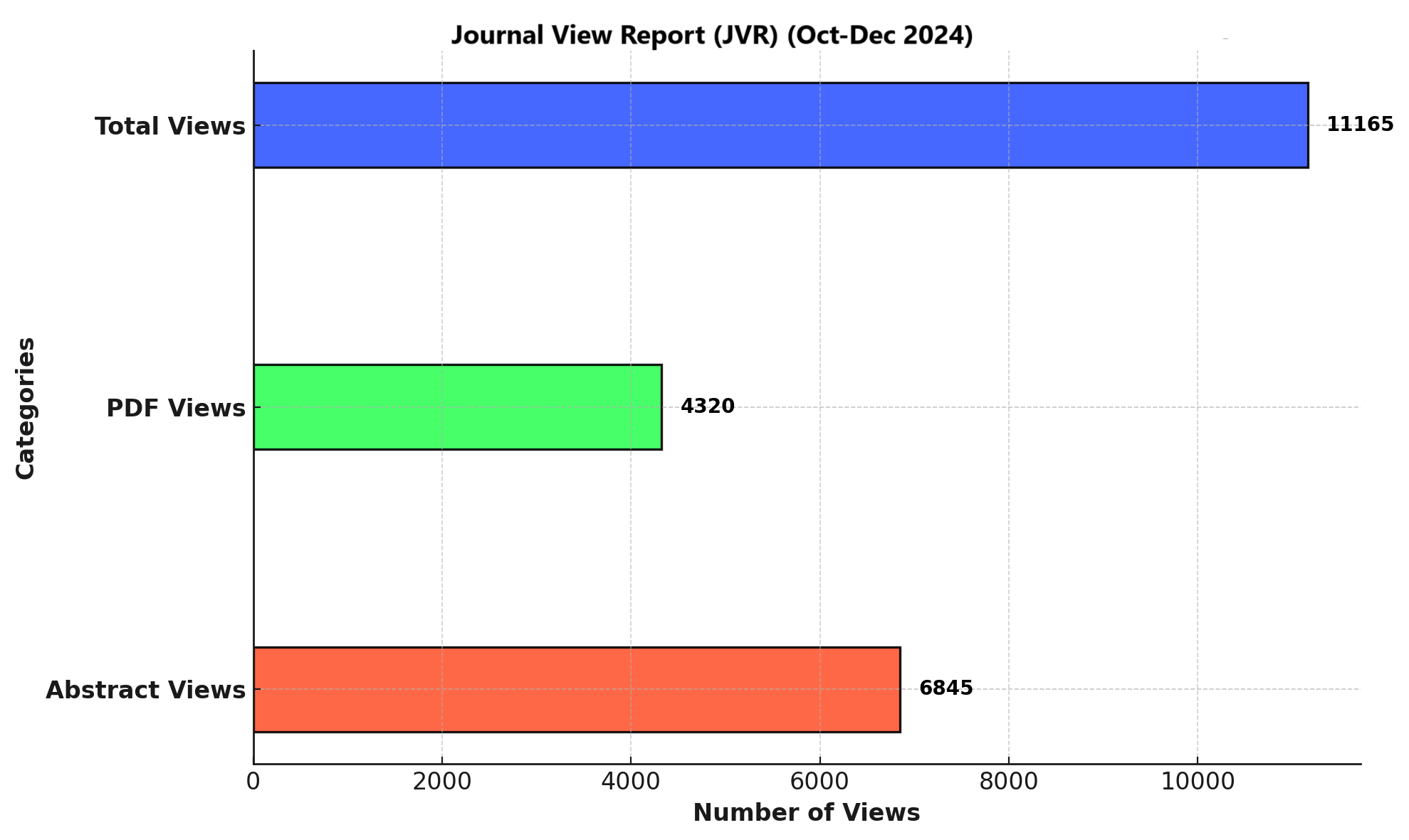
Results: Among 131 AMI patients, 19 (14.5%) exhibited new-onset RBBB. Stratified analysis showed RBBB in 11 of 87 males (12.6%) and 8 of 44 females (18.2%) (p=0.41), and in 13 of 82 patients >50 years (15.9%) versus 6 of 49 aged ≤50 years (12.2%) (p=0.57). Diabetics showed a frequency of 17.6% compared to 12.5% in non-diabetics (p=0.43), while hypertensives had a rate of 16.7% versus 11.3% in non-hypertensives (p=0.47). No statistically significant associations were observed across BMI, socioeconomic class, or residential status.
Conclusion: New-onset RBBB was observed in a clinically relevant portion of AMI patients. Although no significant associations were found with baseline variables, the patterns suggest a possible link warranting further exploration in larger, outcome-based multicenter studies.
References
Michaud K, Basso C, d'Amati G, Giordano C, Kholová I, Preston SD, et al. Diagnosis of myocardial infarction at autopsy: AECVP reappraisal in the light of the current clinical classification. Virchows Arch. 2020;476(2):179-94.
Buja LM. Pathobiology of myocardial ischemia and reperfusion injury: models, modes, molecular mechanisms, modulation, and clinical applications. Cardiol Rev. 2023;31(5):252-64.
Lupu L, Taha L, Banai A, Shmueli H, Borohovitz A, Matetzky S, et al. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardial infarction patients. Clin Cardiol. 2022;45(4):359-69.
keda T. Right bundle branch block: current considerations. Curr Cardiol Rev. 2021;17(1):24-30.
Hassine M, Kallala MY, Jamel A, Bouanene I, Bouchahda N, Mahjoub M, et al. The impact of right bundle branch block and SIQIII-type patterns in determining risk levels in acute pulmonary embolism. F1000Res. 2023; 12:545-9.
Basit H, Kahn A, Zaidi S, Chadow H, Khan A. A case of ST-elevation myocardial infarction with right bundle branch block, an ominous sign of critical coronary occlusion. Cureus. 2022;14(1): e21216-9.
Ardiana M, Sufiyah IM, Hamdani MN. Right bundle branch block evolving to myocardial ischemia in a patient with chronic middle back pain: a case report. J Med Case Rep. 2023;17(1):149-52.
Rehman S, Rahim A, Ali J, Sajjad W, Bilal A, Ullah R, et al. Frequency of new onset right bundle branch block in acute myocardial infarction and its coronary angiographic findings in patients presenting at Tertiary Care Hospital, Peshawar. Pak J Cardiovasc Interv. 2022;2(1):28-34
Figueroa-Triana JF, Mora-Pabón G, Quitian-Moreno J, Álvarez-Gaviria M, Idrovo C, Cabrera JS, et al. Acute myocardial infarction with right bundle branch block at presentation: Prevalence and mortality. J Electrocardiol. 2021;66:38-42.
Galcerá-Jornet E, Consuegra-Sánchez L, Galcerá-Tomás J, Melgarejo-Moreno A, Gimeno-Blanes JR, Jaulent-Huertas L, et al. Association between new-onset right bundle branch block and primary or secondary ventricular fibrillation in ST-segment elevation myocardial infarction. Eur Heart J Acute Cardiovasc Care. 2021;10(8):918-25.
Basit H, Kahn A, Zaidi S, Chadow H, Khan A. A Case of ST-Elevation Myocardial Infarction With Right Bundle Branch Block, an Ominous Sign of Critical Coronary Occlusion. Cureus. 2022;14(1):e21216.
Littmann L. Common ECG interpretation software mistakes. Part I: False reporting of myocardial infarction. J Electrocardiol. 2023;81:32-5.
Nikus K, Birnbaum Y, Fiol-Sala M, Rankinen J, de Luna AB. Conduction Disorders in the Setting of Acute STEMI. Curr Cardiol Rev. 2021;17(1):41-9.
Khawaja M, Thakker J, Kherallah R, Ye Y, Smith SW, Birnbaum Y. Diagnosis of Occlusion Myocardial Infarction in Patients with Left Bundle Branch Block and Paced Rhythms. Curr Cardiol Rep. 2021;23(12):187.
Meyer MR, Radovanovic D, Pedrazzini G, Rickli H, Roffi M, Rosemann T, et al. Differences in presentation and clinical outcomes between left or right bundle branch block and ST segment elevation in patients with acute myocardial infarction. Eur Heart J Acute Cardiovasc Care. 2020;9(8):848-56.
Shrivastav R, Perimbeti S, Casso-Dominguez A, Jneid H, Kwan T, Tamis-Holland JE. In Hospital Outcomes of Patients With Right Bundle Branch Block and Anterior Wall ST-Segment Elevation Myocardial Infarction (From a Nationwide Study Using the National Inpatient Sample). Am J Cardiol. 2021;140:20-4.
Pérez-Riera AR, Barbosa-Barros R, Andreou AY, Fiol-Sala M, Birnbaum Y, da Silva Rocha M, et al. Left septal fascicular block: Evidence, causes, and diagnostic criteria. Heart Rhythm. 2023;20(11):1558-69.
Xenogiannis I, Kolokathis F, Alexopoulos D, Rallidis LS. Myocardial infarction due to left main coronary artery total occlusion: A unique electrocardiographic presentation. J Electrocardiol. 2023;76:26-31.
Macfarlane PW. New ECG Criteria for Acute Myocardial Infarction in Patients With Left Bundle Branch Block. J Am Heart Assoc. 2020;9(14):e017119.
Birnbaum Y, Ye Y, Smith SW, Jneid H. Rapid Diagnosis of STEMI Equivalent in Patients With Left Bundle-Branch Block: Is It Feasible? J Am Heart Assoc. 2021;10(18):e023275.
Lee WC, Fang YN, Chen TY, Hsieh YY, Tsai YH, Fang HY, et al. The Relationship of Conduction Disorder and Prognosis in Patients with Acute Coronary Syndrome. Int J Clin Pract. 2022;2022:9676434.
Rector G, Triska J, Ajene G, Wang A, Haddadin F, Jabri A, et al. Right Bundle Branch and Bifascicular Blocks: Insensitive Prognostic Indicators for Acute Myocardial Infarction. Curr Probl Cardiol. 2023;48(1):101418.
Senftinger J, Sörensen NA, Blankenberg S, Clemmensen P. Right bundle branch block in suspected acute coronary syndromes: Diagnostic challenges, treatment and prognosis. J Electrocardiol. 2024;87:153824.

Downloads
Published
Issue
Section
License
Copyright (c) 2025 Atif Kamal, Tariq Nawaz, Sher Ali Khan, Waseem Iqbal, Saddam Hussain, Roman Khan (Author)

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.