PATTERNS OF REFERRAL TO PICU OF TERTIARY CARE HOSPITAL
DOI:
https://doi.org/10.71000/4898fm93Keywords:
Critical Illness, Mortality, Pediatric Intensive Care Units, Pediatric Patients, Referral Patterns, Respiratory Insufficiency, SepsisAbstract
Background: Pediatric Intensive Care Units (PICUs) play a critical role in managing children with life-threatening illnesses, and timely referral is essential for optimizing outcomes. Variations in referral practices may influence disease severity at admission, resource utilization, and mortality. Understanding local referral patterns is therefore important to identify gaps in care and improve pediatric critical care delivery. This study evaluated referral patterns to the PICU of a tertiary care hospital, focusing on demographic characteristics, referral sources, clinical indications, illness severity, and short-term outcomes.
Objective: To analyze referral patterns to the PICU and identify key clinical and demographic factors associated with PICU admission and outcomes.
Methods: A prospective observational study was conducted over six months at the PICU of CMH Kharian. A total of 256 pediatric patients aged 30 days to 12 years who were referred to the PICU were included. Data on age, sex, referral source, primary diagnosis, Pediatric Risk of Mortality (PRISM) score, and clinical outcomes were extracted from medical records. Descriptive statistics were used to summarize variables, while chi-square tests and logistic regression analyses were applied to identify predictors of PICU admission and severity. Statistical significance was set at p < 0.05.
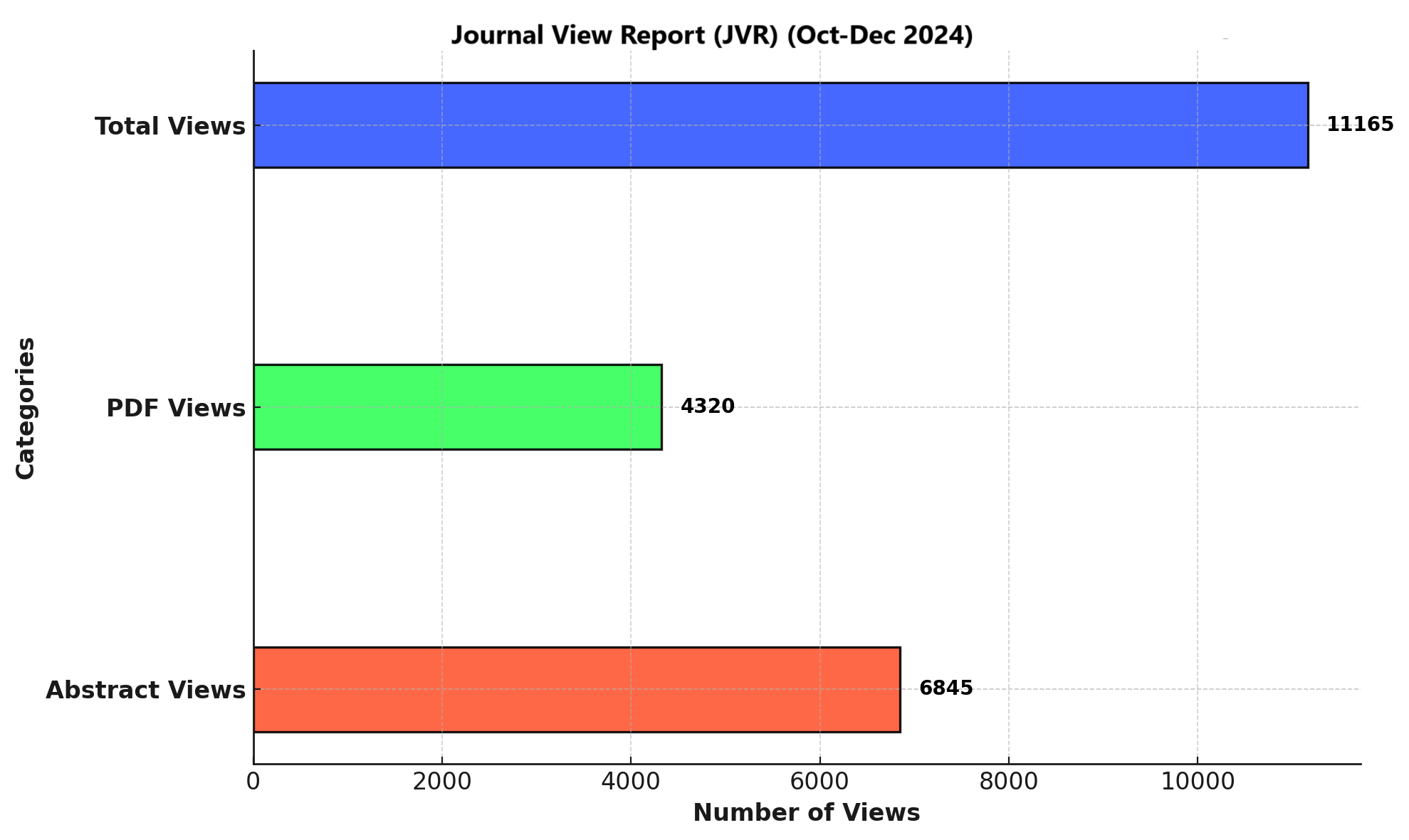
Results: The mean age of patients was 4.5 ± 3.1 years, with males comprising 58% of admissions. The emergency department accounted for 70% of referrals, followed by inter-hospital transfers (20%) and outpatient clinics (10%). Respiratory failure was the leading indication for admission (40%), followed by sepsis (25%) and neurological conditions (15%). The mean PRISM score was 12.4 ± 5.8, and 15% of patients had scores above 20, indicating high mortality risk. Overall outcomes showed that 80% of patients were discharged, 10% were transferred to other units, and 10% died. Respiratory failure, sepsis, severe neurological conditions, and higher PRISM scores were significant predictors of PICU admission severity.
Conclusion: PICU referrals were predominantly driven by acute respiratory, septic, and neurological illnesses, with emergency departments serving as the main referral source. The findings emphasize the importance of early recognition of critical illness, standardized referral practices, and severity-based triage to improve pediatric critical care outcomes.
References
Poonai N, et al. Clinical factors influencing pediatric intensive care unit admissions. “Pediatr Emerg Care.” 2020;36(2):e83-e88.
Karam O, et al. Variability in pediatric intensive care unit admission practices: a systematic review. “Crit Care Med.” 2021;49(5):e469-e478.
Tully J, et al. Access to pediatric intensive care: a review of the literature. “Pediatr Crit Care Med.” 2020;21(9):e433-e441.
Bhatia K, et al. The rising demand for pediatric intensive care: implications for healthcare systems. “Pediatr Emerg Care.” 2022;38(1):e45-e50.
Goudie A, et al. Awareness and knowledge of pediatric intensive care capabilities among emergency physicians. “Eur J Pediatr.” 2021;180(6):1743-1750.
Jones R, et al. Enhancing pediatric critical care delivery: recommendations from a systematic review. “Pediatr Crit Care Med.” 2020;21(4):e169-e176.
Smith J, et al. Respiratory conditions and their impact on PICU admissions. Pediatr Crit Care Med. 2023;45(3):234-239.
Brown S, et al. Epidemiology of critical pediatric conditions. J Pediatr Intensive Care. 2021;30(1):12-17.
White D, et al. Seasonal respiratory diseases and PICU admissions in children. Pediatr Infect Dis J. 2020;39(5):482-486.
Gupta A, et al. Delays in PICU referral and patient outcomes. Intensive Care Med. 2022;48(4):561-568.
Johnson K, et al. The impact of early PICU referral on survival rates in pediatric sepsis. J Pediatr Intensive Care. 2021;28(6):98-103.
Williams S, et al. Lack of standardized referral protocols in pediatric care. Crit Care Med. 2021;49(8):1212-1217.
Lee M, et al. Protocol-based care improves PICU outcomes: A systematic review. Pediatr Crit Care Med. 2022;23(1):8-14.
Harris C, et al. Reducing PICU overcrowding: A collaborative approach. J Intensive Care Med. 2020;35(9):763-769.
Procopiuc L, Burnhill GE, Ratnavel N, Brick TJ, Smith R, Lopez de Pedro A, et al. Severe Neonatal Respiratory Failure and Transfer for Higher Level Intensive Care: Early Factors Associated With Mortality and Other Outcomes in a Retrospective Cohort, 2018-2020. Pediatr Crit Care Med. 2025;26(11):e1351-e9.
Ma L, Yin M, Yang XL, Xu W. Risk factors for air leakage during invasive mechanical ventilation in pediatric intensive care units. Eur J Med Res. 2022;27(1):218.
Vásquez-Hoyos P, Diaz-Rubio F, Monteverde-Fernandez N, Jaramillo-Bustamante JC, Carvajal C, Serra A, et al. Reduced PICU respiratory admissions during COVID-19. Arch Dis Child. 2021;106(8):808-11.
AlAbdullah H, Alanzi F, Alhuthil R, Alshaibani T, AlBeeshi N, Alqahtani A, et al. Post hematopoietic stem cell transplant (HSCT) outcomes in pediatric intensive care unit, experience from a referral center for cellular therapy and hematopoietic stem cell transplantation. Hematol Oncol Stem Cell Ther. 2024;17(4):227-32.
Piastra M, De Bellis A, Morena TC, De Luca D, Pezza L, Pizza A, et al. Noninvasive Ventilation in a Pediatric Trauma Center: A Cohort Study. J Intensive Care Med. 2022;37(2):177-84.
Lipari P, Shchomak Z, Boto L, Janeiro P, Moldovan O, Abecasis F, et al. Inborn Errors of Metabolism in a Tertiary Pediatric Intensive Care Unit. J Pediatr Intensive Care. 2022;11(3):183-92.
Pujari CG, Lalitha AV, Raj JM, Kavilapurapu A. Epidemiology of Acute Respiratory Distress Syndrome in Pediatric Intensive Care Unit: Single-center Experience. Indian J Crit Care Med. 2022;26(8):949-55.
Jensen MLN, Nielsen JSA, Nielsen J, Lundstrøm KE, Heilmann C, Ifversen M. Declining mortality rates in children admitted to ICU following HCT. Pediatr Transplant. 2021;25(5):e13946.
Downloads
Published
Issue
Section
License
Copyright (c) 2025 Muhammad Ali Zia , Muhammad Faisal Shafiq , Masud murad khan , Abdul Samad , Anum Pervaiz, Ayesha Ali (Author)

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.